The main steps of ART are –
1) Image acquisition – ART needs adequate information of tumor, OAR delineation, and accurate dose calculation which is possible with sufficient image quality of CBCT (iterative).
2) Deformable Image Registration (DIR) – This is an important step in ART to account for changes in the shape and size of internal organs between initial and adaptive planning images. The images are usually acquired at every fraction prior to treatment delivery to perform tasks such as deforming contours and electron density mapping. It helps in contour propagation, plan adjustment and fractional dose accumulation. There are various qualitative and quantitative measures for evaluating the image registration accuracy to reduce errors.
3) Dose accumulation and tracking– As the anatomy and corresponding contours change, the initial dose calculated using the planning data set may have limited accuracy and may not represent the actual dose delivered. ART provides summary of delivered dose, by voxel by voxel dose accumulation for each delivery time point. This “dose of the day “ is warped back to initial planning CT scan for dose accumulation over the total fractions to date. The methodology of deforming adaptive planning image yields improved dose estimation.
4) Rapid Replanning – Replanning cases for ART involves consideration of stratgegy ( online vs offline), delineation of targets and OARs, time taken for replanning and clinical criteria for adaptation.
5) Pre treatment planning and delivery quality assurance – Offline ART strategies follow standard treatment plan and delivery QA approaches that EBRT planning workflow. Online ART needs automated plan check and secondary dose calculation tools for independent evaluation of plan quality.
Raysearch even helps with artificial intelligence (AI) in various components of ART, like auto-contouring and autosegmentation, registration, planning and quality assurance. Raysearch is enabled with model based and atlas based segmentation which has the capability of machine learning.
We at Mahatma Gandhi Cancer Hospital & Research Centre are mainly focusing on lung, head and neck, prostate and cervical cancers to improve therapeutic ratio with Adaptive Radiotherapy.
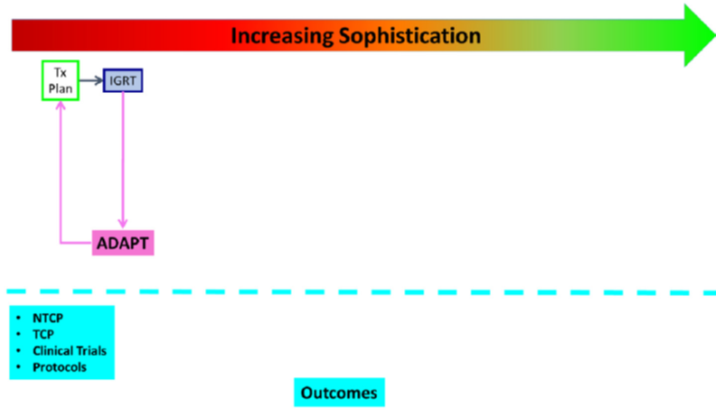
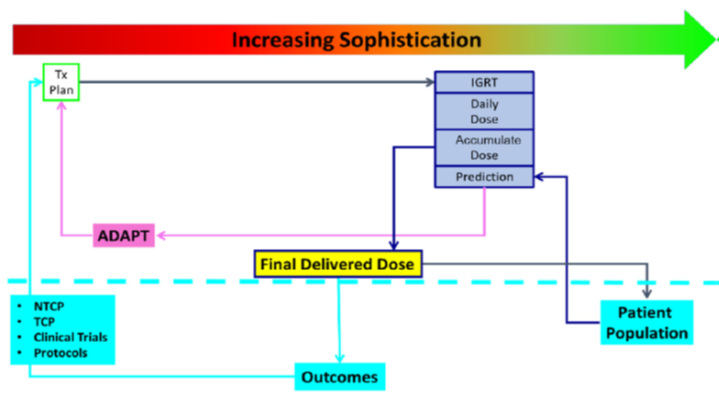
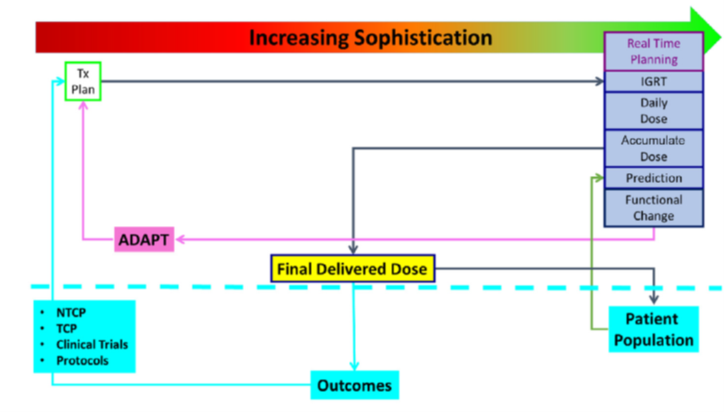
Fig 1 : Flowchart showing increased levels of adaptive radiotherapy, ranging from simple IGRT based replanning to DIR based dose accumulation and development of predictive models tied to an outcome database
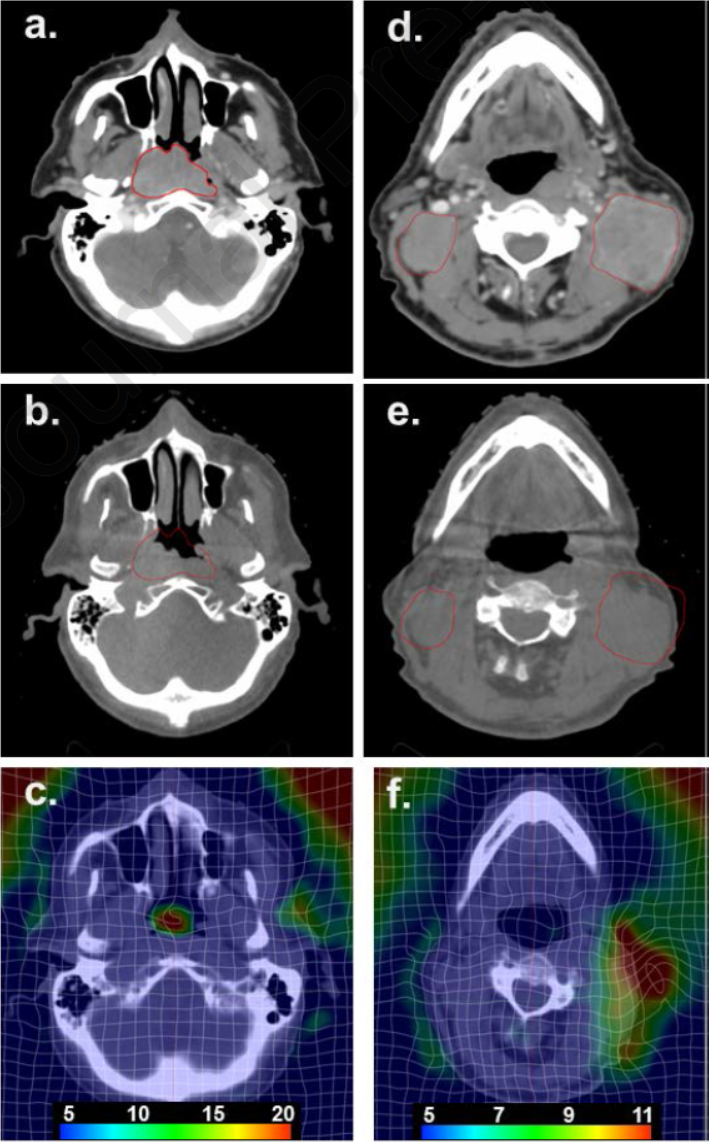
A&D – represent the primary nasopharyngeal tumor and neck nodes prior to starting RT. B&D represents shrinkage of primary and nodes after 12 fractions. C& F represents deformation of image to propagate the contours and dose for adaptive plan.